


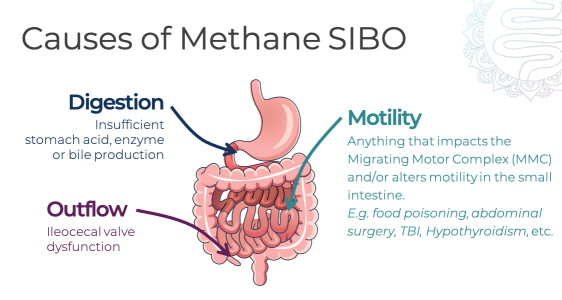
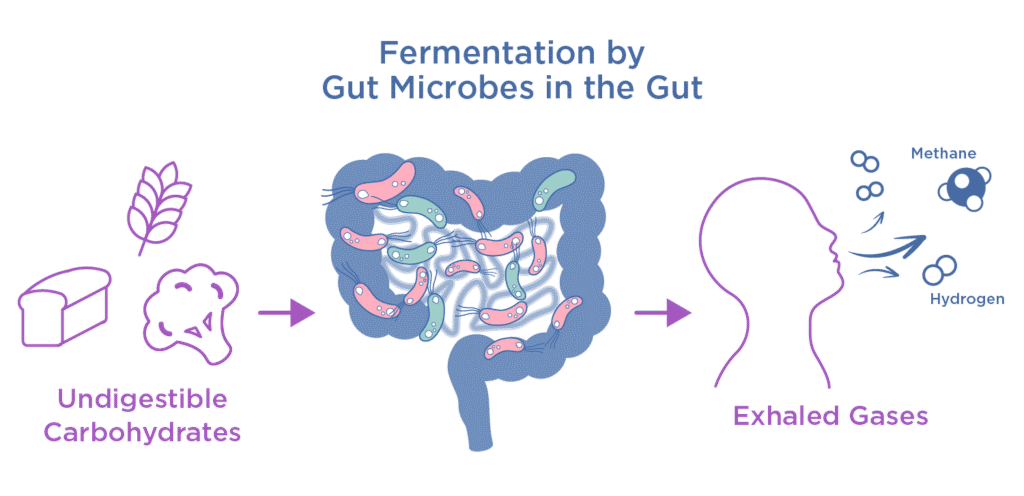
Chronic constipation and SIBO/IMO affect up to 20% of adults globally. These disorders often result from gut hypomotility driven by methanogenic archaea. Breath methane offers a non-invasive biomarker to flag this condition early. Clinicians rely on accurate methane (CH₄) quantification to guide treatment and improve patient outcomes. Without precise data, patients face guesswork therapies and lingering discomfort.
However, conventional electrochemical and metal oxide sensors struggle with low-level CH₄ detection. Most MOx devices detect methane above 2 ppm, and optical sensors start at 100 ppm. This sensitivity gap yields false negatives in early or mild cases. Consequently, clinicians miss methanogen-driven hypomotility and delay targeted therapy. We need sub-ppm accuracy to close this diagnostic gap.
Tunable Diode Laser Absorption Spectroscopy (TDLAS) methane analyzers deliver sub-ppb sensitivity and robust analytical performance, enabling precise breath Methane (CH₄) quantification that closes diagnostic gaps in chronic constipation and Small Intestinal Bacterial/Intestinal Methanogen Overgrowth (SIBO/IMO).
What Are the Clinical Utility and Diagnostic Thresholds of Breath Methane Testing?
Firstly, breath methane levels guide intestinal methanogen overgrowth diagnosis. Industry consensus defines CH₄ ≥ 10 ppm at any time as positive for IMO. This threshold stems from animal and human studies linking CH₄ to transit delay. For example, the North American Consensus sets 10 ppm as the cut-off for methane positivity in breath tests. Clinicians rely on this clear biomarker threshold to flag patients for targeted therapy.
Furthermore, quantitative methane links directly to constipation risk and guides therapy. A meta–analysis of 1,277 subjects found methane producers had a 3.51–fold higher odds of constipation–predominant IBS or functional constipation. Clinicians then use CH₄ levels to tailor treatment, such as:
- Antibiotic Selection: Combine rifaximin with neomycin to eradicate methane producers (85% response rate).
- Prokinetic Adjuncts: Add agents like prucalopride or tegaserod when methane persists.
This data empowers gastroenterologists to match interventions with breath test results and improve patient outcomes.
How Does Methane Gas Analyzers Achieve Precise Breath Methane Measurement?
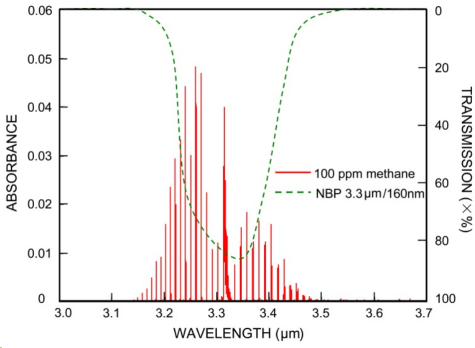
TDLAS relies on tunable diode lasers that target methane’s unique absorption lines. By sweeping the laser wavelength across specific CH₄ spectral features, the TDLAS methane gas analyzers isolate methane from other breath gases. This direct probing yields unmatched selectivity, even in complex biological matrices. Moreover, it reaches a detection limit of customizable ppm to ppb, letting clinicians catch subtle methane rises that older tests miss. In short, TDLAS acts like a molecular fingerprint scanner, pinpointing methane with surgical precision.
At its core, the methane gas analyzers combine four key modules:
- Laser Source: A tunable diode laser emits a narrow, stable beam.
- Multipass Cell: Mirrors fold the beam path, boosting interaction length.
- Photodetector: Captures light after CH₄ absorption events.
- Digital Signal Processor (DSP): Converts analog signals into real-time methane concentration data.
Next, the methane gas analyzers deliver industry-leading specs that support clinical decision-making:
- Dynamic Range & Sensitivity: 0–5000 ppb; Min Detection Limit ≤ 5 ppb; customizable ppm.
- Accuracy & Repeatability: ≤ ± 0.3% Full-Scale; ≤ 0.2% FS
- Stability & Response: 72 h zero drift ≤ ± 0.5% FS; span drift ≤ ± 1.0% FS; T₉₀ ≤ 60 s
Moreover, a 1 s sampling interval supports near-real-time breath monitoring. Together, these features empower gastroenterologists to detect subtle methane shifts, tailor interventions, and track treatment response dynamically.
How to Implement Methane Gas Analyzers in Clinical Practice?

To roll out TDLAS-based breath methane gas analyzers, follow a four-step roadmap that ensures accuracy and clinical compliance. It covers sampling protocol, data integration, calibration & QA/QC, and staff training.
1. Sampling Protocol
First, standardize the substrate to lactulose or glucose. Then enforce a 12-hour fasting baseline to minimize background interference. Next, collect breath samples every 15 minutes over a three-hour window. Label and timestamp each sample for traceability. This consistent approach reduces variability and boosts diagnostic confidence.
2. Data Integration
Next, set the methane gas analyzers to record methane levels at one-second intervals. Use the digital output to stream data directly into the HIS/EMR. Automate report generation to flag CH₄ spikes above 10 ppm instantly. Moreover, dashboards can track patient trends and treatment response over time. Real-time integration speeds decision-making and enhances clinical workflows.
3. Calibration & QA/QC
Additionally, exploit the methane gas analyzers’ low drift specs to schedule zero/span calibrations bi-weekly. Specifically, run zero drift checks within ± 0.5% FS and span checks within ± 1.0% FS. Embedding these tasks into SOPs meets lab accreditation and reduces instrument downtime. This proactive QA/QC approach safeguards long-term data integrity.
4. Training & Competency
Finally, develop a modular curriculum covering laser safety, instrument operation, and data interpretation. Incorporate hands-on workshops for sample handling and troubleshooting. Assess competency with practical exams and periodic audits. This structured training builds team confidence and maintains high-quality testing standards.
What Economic Benefits and Reimbursement Opportunities Does Methane Gas Analyzers Offer?

1. Cost–Benefit Analysis
Moving beyond technical performance, let’s examine the economic case for TDLAS methane gas analyzers. Although the upfront capital expenditure exceeds that of conventional sensors, the return on investment materializes quickly through:
- Fewer Repeat Tests: Precise CH₄ detection cuts false negatives and saves on repeat breath assays.
- Optimized Antibiotic Stewardship: Quantitative data guides targeted rifaximin + neomycin therapy, reducing drug waste and adverse events.
- Shorter Diagnostic Cycles: Real-time results accelerate clinical decision-making and increase lab throughput.
Together, these factors shrink operational costs and deliver a strong ROI over the methane gas analyzers’ lifecycle.
2. Reimbursement Landscape
Furthermore, reimbursement drives clinical adoption. The hydrogen/methane breath test falls under CPT code 91065, which payers recognize for SIBO, IMO, and lactose malabsorption diagnostics medibillmd. To secure coverage and minimize denials:
- Verify Coverage: Confirm payer policies for CPT 91065 before ordering.
- Preauthorization & Documentation: Submit medical necessity with relevant ICD-10 codes and clinical notes.
- Leverage Real–World Evidence: Present patient outcome data to negotiate higher reimbursement rates.
By aligning testing protocols with existing billing frameworks, clinics can enhance adoption and ensure sustainable revenue.
What Does the Future Hold for Methane Gas Analyzers in Breath Testing?
(Remote_Health_Monitoring)
TDLAS methane analyzers deliver high selectivity and sub-ppb sensitivity. They respond in under 60 seconds and pinpoint methanogenic overgrowth with laser-sharp accuracy . Moreover, they reduce misdiagnoses and eliminate repeat tests. Digital output and real-time integration streamline workflows. Importantly, quantifying CH₄ guides personalized antibiotic and prokinetic regimens. According to ESEGAS, the methane gas analyzers offer a customizable % to ppb range, and T90 ≤ 60 s. Finally, adopting this turnkey solution boosts diagnostic confidence and patient outcomes.
Looking ahead, innovators should explore three key directions to personalize gut health management:
- Point–of–Care Miniaturization: Shrink TDLAS modules for in-clinic or at-home use.
- Multi–Omics Integration: Combine breath CH₄ data with microbiome and metabolome profiles for deeper insights.
- Remote Monitoring: Link portable analyzers to cloud platforms for continuous patient tracking and telehealth interventions.
By advancing along these paths, we can tailor therapies, improve outcomes, and redefine how we manage gut motility disorders.
Ready to elevate your gastroenterology practice? Contact an ESEGAS solution expert today to schedule a demo and start precision care for chronic constipation and SIBO/IMO.




















